Chapter 12 : Asystole – Understanding H’s and T’s
Asystole is associated with the absence of cardiac electrical activity, contraction of the heart muscle, and cardiac output. “Flatline” is a term used for no electrical activity seen on the ECG. However, “flatline” can result from other causes such as:
- Leads are properly connected
- Power unit is on
- Signal gain/amplitude/strength is not turned down or too low
- The rhythm doesn’t look like another pattern
Asystole ACLS Training Video:
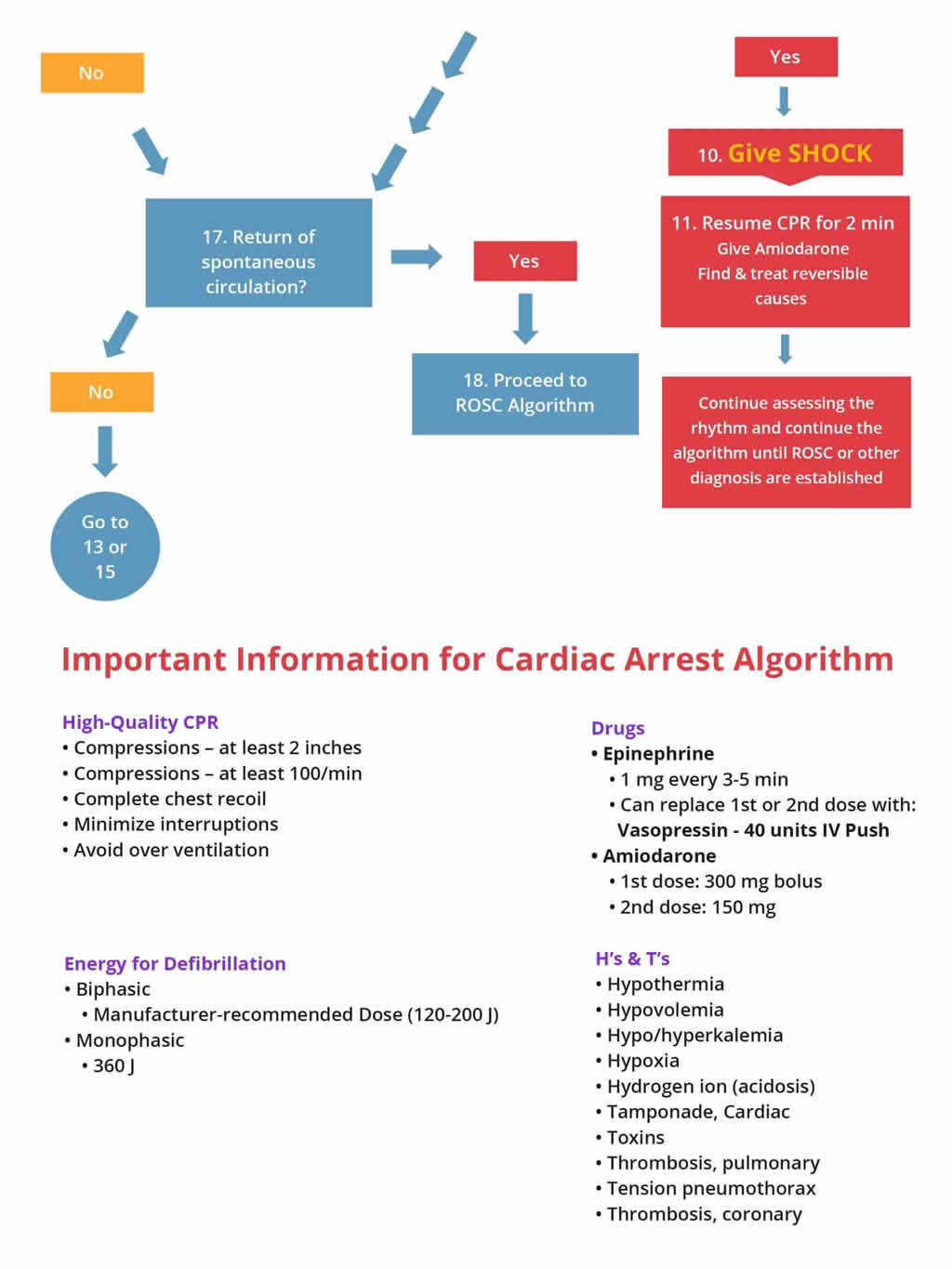
Asystole can be caused by many factors and are represented as H’s and T’s:
| H’s |
T’s |
| Hypovolemia – Decreased blood volume |
Tension pneumothorax – air in the pleural space around the lung (lung collapses) |
| Hypoxia- decreased partial pressure of oxygen in blood |
Tamponade – compression of the heart produced by excess fluid surrounding the heart |
| Hydrogen ion (acidosis) – Increase in the concentration of H ions in blood |
Toxins – poisonous substances |
| Hyper-/hypokalemia –abnormally high or low potassium concentration in the blood |
Thromobosis (pulmonary) – formation of a blood clot which blocks a blood vessel in lungs |
| Hypothermia – body temperature less than 30 degrees C (86 degrees F) |
Thrombosis (coronary) –formation of a blood clot which blocks a blood vessel in heart |
Scenario: You are a paramedic and arrive on the scene. A man is lying on the floor unconscious and the neighbor tells you that she saw the man collapse as he was unlocking his front door.
Assessment:
- Check for responsiveness – Tap and shout “Are you alright?” and look at chest for movement.
- Check carotid pulse and note no pulse is present
Interventions:
- If no pulse, immediately start compressions at a rate of 100 compressions per minute and allow chest to recoil. 30 compressions to 2 breaths.
- Prepare to transport patient to the nearest hospital, while continuing effective Cardiopulmonary Resuscitation (CPR).
- Attach monitor and check for shockable rhythm, if no shockable rhythm present, the patient is in asystole or PEA, start CPR for 2 mins and obtain IV/IO access.
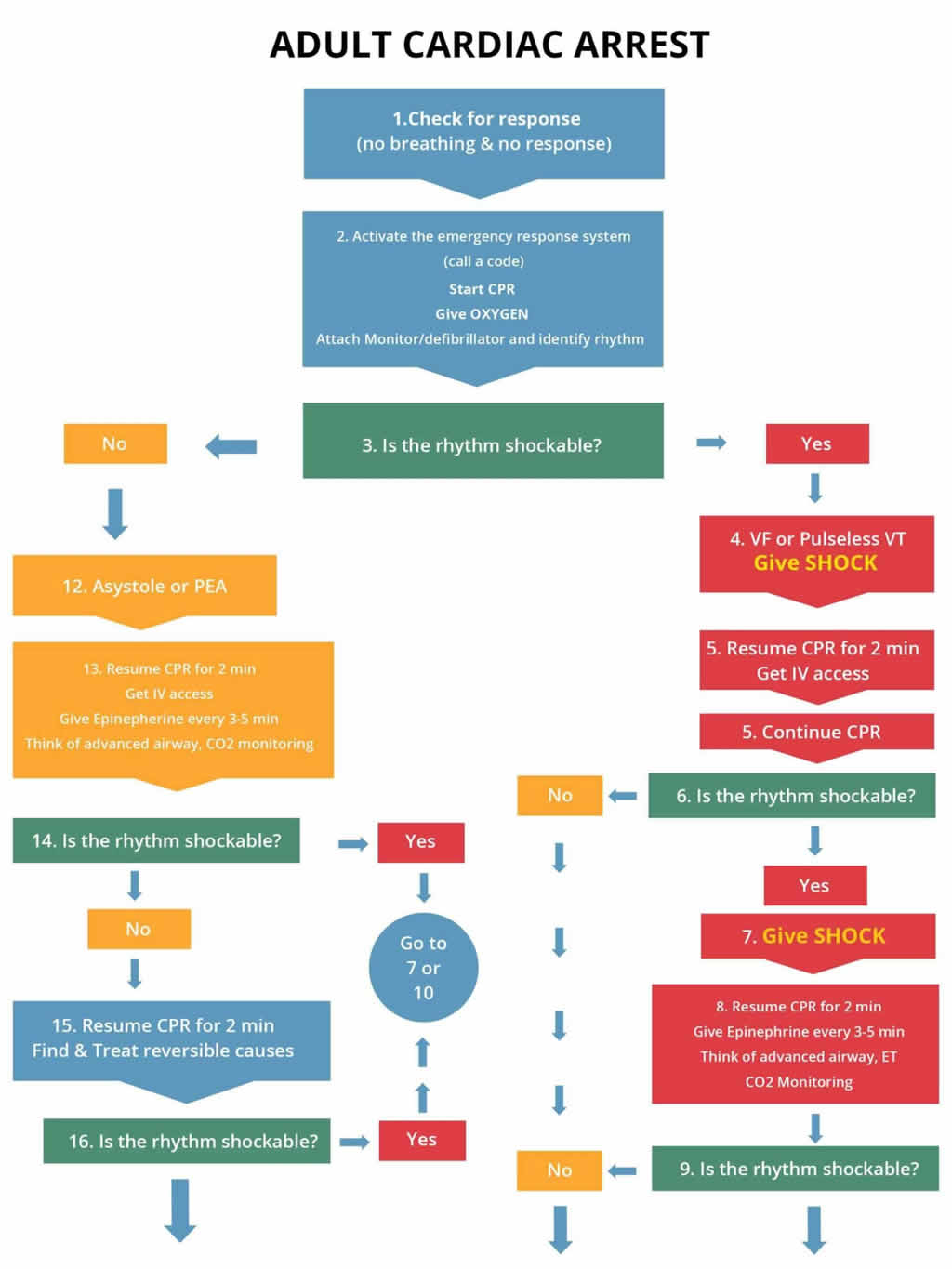
Management: AT the hospital initiate the cardiac arrest algorithm on the right if the patient still has no pulse and does not respond to BLS. Get a code team in place.
- Once IV/IO access is obtained give the following drugs:
- Epinephrine 1 mg IV/IO and repeat every 3 to 5 minutes
- Maintain advanced airway and capnography if needed.
- Pause and check for shockable rhythm. If not shockable, continue CPR for 2 minutes and try to treat the reversible causes
The following is an algorithm shows management of cardiac arrest due to a flat line situation or asystole/PEA (left side of chart)
Note: When conducting the BLS and ACLS survey on a patient with asystole, there may be times when you should hold resuscitative efforts; those include:
- Signs of irreversible death like rigor mortis
- DNAR – Do Not Attempt Resuscitation
- Threat to safety of the providers
- Living Will/Family Wishes
Learning Outcomes:
You have completed Chapter XII. Now you should be able to:
- Apply the Cardiac Arrest Algorithm to Asystole
- Recognize asystole in a patient
- Understand the H’s & T’s in relation to Asystole/PEA
- Understand when it is necessary to hold resuscitation
- Understand the treatments used in Asystole



