Chapter 14 : Bradycardia ACLS
Bradycardia is defined as a heart rate of less than 60 beats per minute. Symptomatic bradycardia and the management thereof, is defined as a heart rate less than 50 beats per minute. Causes of bradycardia include:
- Hypertension
- Congenital heart defect
- Tissue damage due to aging, heart disease or heart attack
- Myocarditis
- Hypothyroidism
- Imbalance of electrolytes
- Obstructive sleep apnea
- Inflammatory diseases
- Medicationst
Bradycardia ACLS Video:
Symptoms of bradycardia include:
- Dizziness
- Shortness of breath
- Feeling tired
- Chest pain or fluttering of heart
- Confused and trouble concentrating
- Drop in blood pressure causing the person to faint
- Presyncope – lightheadedness
- Syncope – loss of consciousness
Signs of bracycardia include:
- Hypotension – low blood pressure
- Orthostatic hypotension – a drop in blood pressure due to change in position (example: sitting or standing)
- Diaphoresis – sweating
- Pulmonary congestion or edema – increase of fluid in the lungs
- Congestive heart failure – heart does not pump enough blood
- Premature Ventricular contractions (PVCs) – Ventricle produces abnormal heart beats
There are 4 types of ECG rhythms associated with bradycardia:
- Sinus bradycardia
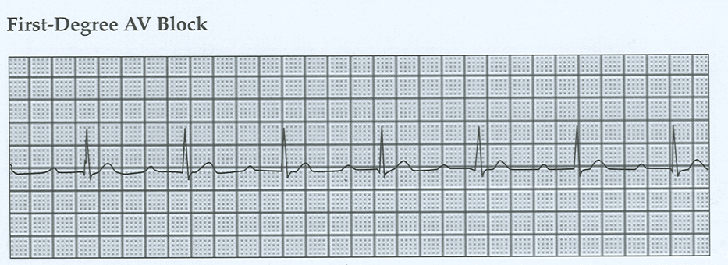
- First-degree AV block
- Second-degree AV block: Type I (Mobitz 1) and Type II (Mobitz II)
- Third-degree AV block
Sinus bradycardia starts in the SA node with decreased rate (<60 beats/min).

First degree AV block is when the PR interval is prolonged (> 0.20 seconds).
2nd Degree AV block type I (Wenckebach-Mobitz I) is when the PR interval becomes increasingly prolonged, R-R intervals are shortened, and a beat (QRS) finally drops
2nd degree AV block Type II (Mobitz II) is when there is no change in the PR interval and than a beat will drop.

3rd degree Av block is a complete heart block where the P wave and QRS complexes are not connected.
Scenario: You are a paramedic who arrives at a house of the patient who has collapsed. The wife tells you that her husband was having difficulty breathing at first, but then grabbed his chest and collapsed.
Assessment:
- Check for responsiveness – Tap and shout “Are you alright?” and look at chest for movement. Check carotid pulse and note there is pulse and breathing
- Prepare to transport patient to the nearest hospital
- Hook the patient to the monitor and identify the rhythm as bradycardia (<50 beats/min)
Interventions:
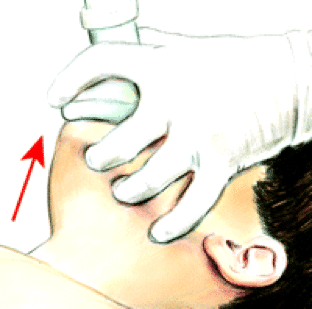
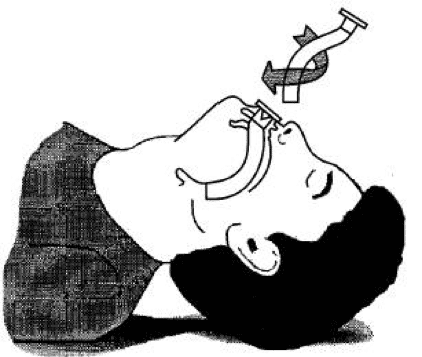
- Maintain airway
- Help with breathing and give oxygen if hypoxemic and monitor O2 saturation
- Monitor BP and HR and conduct a 12-lead ECG and diagnose
- Check for persistent bradyarrhythmia
Management: at the hospital
- If bradyarrhythmia is present, administer atropine (first dose of 1 mg bolus, then repeat 3-5 mins, max of 3 mg)
- If atropine is ineffective, apply transcutaneous pacing or administer Dopamine infusion (5-20 mcg/kg/min) or Epinephrine infusion (2 to 10 mcg/min)
The following is an algorithm showing management of bradycardia in detail.
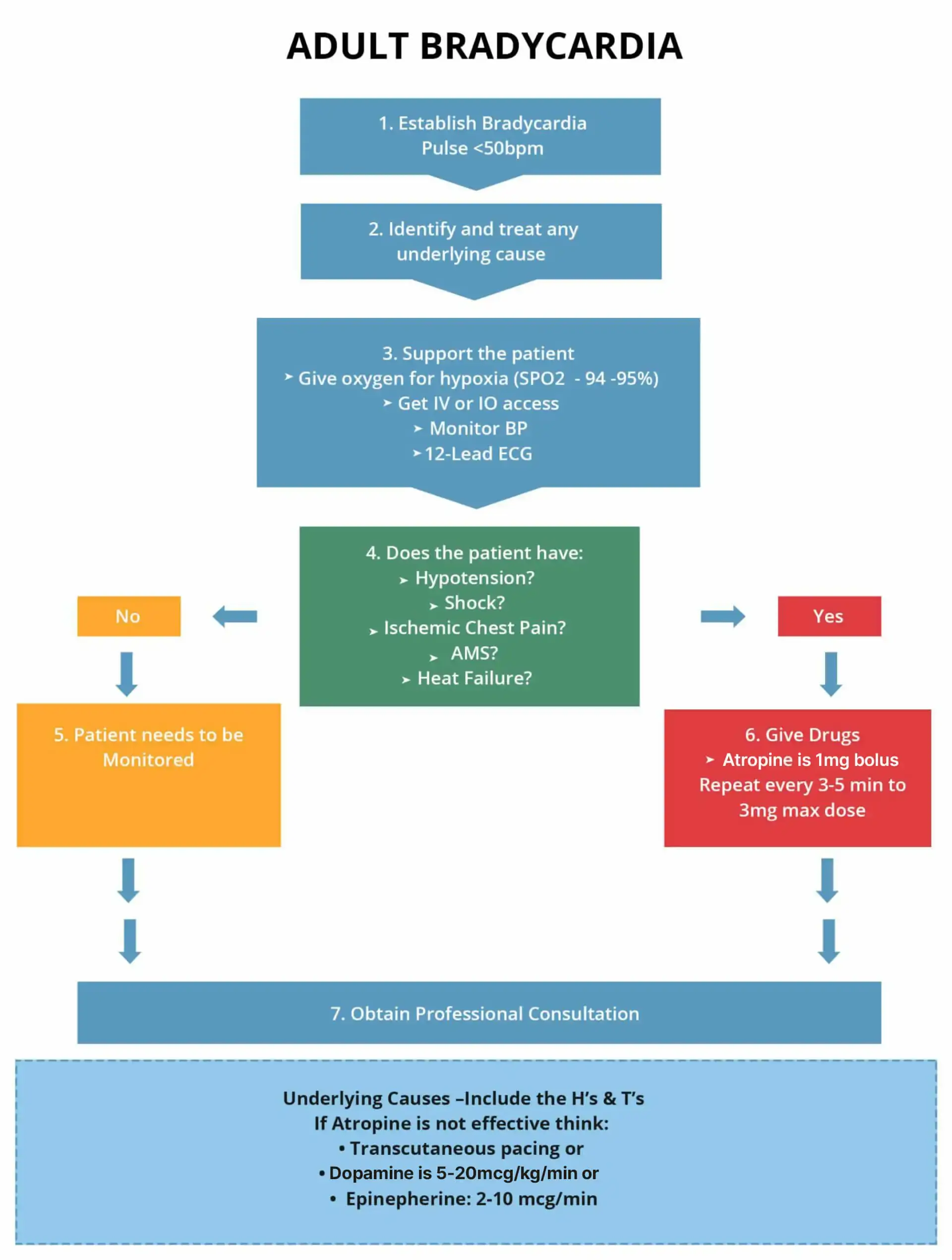
Use Atropine as the first-line therapy for Bradycardia
- Administer atropine –first dose of 1mg bolus, then repeat 3-5 mins, max of 3mg
If atropine does not work:
- Transcutaneous pacing OR
- Dopamine – 5 to 20 mcg/kg/min
- Epinephrine – 2 to 10 mcg/min IV
Transcutaneous pacing is crucial to obtain a normal heart rate again if the patient is showing poor perfusion. Even though atropine is the first line treatment for bradycardia, if the patient has severe symptoms of bradycardia or is crashing then it is critical to start Transcutaneous pacing (TCP).
Start TCP right away if the patient:
- Does not respond to atropine
- Atropine does not work in the patient
- Cannot get IV access or it is taking long
- The patient is deteriorating fast
Once the TCP has started ensure that the heart is getting proper electrical shocks from the pacer. Give analgesics and sedatives to help with pain especially in patients who are alert and awake (might be best to give it before the TCP starts). Make sure to continuously monitor the patient to check if there are any improvements.
REMEMBER: If TCP is ineffective, start infusion of dopamine or epinephrine and get the patient ready for transvenous pacing. Make sure to get professional consultation.
Learning Outcomes:
You have completed Chapter XIV. Now you should be able to:
- Recognize the 4 types of ECG rhythms associated with bradycardia
- Apply the Adult Bradycardia Algorithm
- Understand the signs & symptoms of Bradycardia
- Understand the treatments used in Bradycardia



