Chapter 3: Respiratory Distress And Failure
Respiratory distress can lead to respiratory failure in children that can be life threating and can quickly lead to death. Prompt recognition and management of respiratory distress and failure in infants and children is one of the key components of PALS. Respiratory distress is when the rate and effort of breathing is increased and there are changes seen in airway sounds, skin color and mental status. Respiratory distress can quickly lead to respiratory failure, where there is inadequate oxygenation, ventilation or both and can quickly lead to cardiac arrest.

Lung of a child in respiratory failure and needs respirator for assist ventilation |

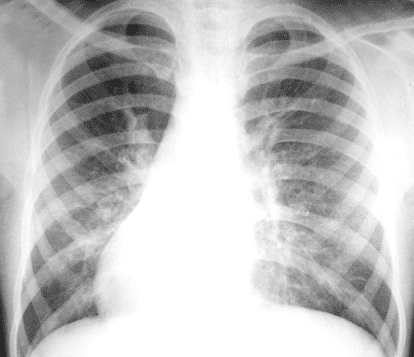
Lung of a child with Respiratory distress syndrome and left sided pneumothorax |
Respiratory Distress And Failure Video:
Hypoxemia or inadequate oxygenation and hypercarbia or inadequate ventilation can lead to respiratory distress and failure. It is important to note that oxygen consumption in infants is 6 to 8 mL/kg per minute, while in an adult it is 4 mL/kg per minute. A pulse oximetry helps indicate if there is decreased oxyhemoglobin saturation in the blood. A SpO2 <94% = hypoxemia. Tissue hypoxia could also be a cause of hypoxemia. It is important to recognize the signs of hypoxia to help distinguish between tissue hypoxia and hypoxemia. The following are signs of tissue hypoxia:
- Tachypnea
- Pallor
- Early tachycardia
- Late bradypnea
- Late bradycardia
- Altered mental status
- Late cyanosis
- Agitation
- Anxiousness
- Nasal flaring
- Fatigue
PALS by American HealthCare Academy Video:
Increased PaCO2 in the blood indicated inadequate alveolar ventilation or hypercarbia. Hypercarbia is more severe, but is harder to detect. The following are signs of hypercarbia:
- Tachypnea
- Altered mental status
- Agitation
- Anxiety
- Nasal flaring
Identification and Management of Respiratory Distress and Failure
Conditions that cause respiratory distress and failure include:
- Upper airway obstruction
- Lower airway obstruction
- Lung tissue disease
- Disordered control of breathing
| Upper Airway Obstruction |
| Anatomy |
Obstruction in the nose, pharynx, or larynx
 |
| Causes |
- Foreign-body aspiration
- Swelling of tissue of upper airway
- Tumor or abscess
- Croup
- Epiglottitis
- Anaphylaxis
- Hypertrophic tonsils
|
| Signs and Symptoms |
- Tachypnea
- Increase in respiration and effort
- Inadequate chest rise and air entry on auscultation
- Stridor
- Change in voice, crying or cough
- Cyanosis
- Drooling
- Increased respiratory rate
|
| Management |
Management of all upper airway obstruction includes:
- Remove object obstructing airway
- Suction mouth or nose
- Reduce airway swelling
- Consider advanced airway or surgery
|
Specific causes of upper airway obstruction include croup and anaphylaxis.
Croup
Croup is a condition where the upper airway is affected due to an acute viral infection. Symptoms include barking cough, stridor and hoarseness. Treatment of croup can vary due to the severity of the disease. Management of croup includes the following:
- Single oral dose of dexamethasone
- Cool mist
- Administration of nebulized racemic epinephrine or L-epinephrine
- Perform endotracheal intubation
- Use of heliox (helium-oxygen mixture)
Anaphylaxis

Anaphylaxis is a type I hypersensitivity allergic reaction that can causes intense bronchoconstriction in which the patient may stop breathing. The following table shows the actions needed for the treatment of anaphylaxis.
| Treatment |
| Give IM epinephrine through the autoinjector – depends on how severe the problem is |
| Think of using endotracheal intubation if there is bronchospasm/wheezing – give albuterol through inhaler or by nebulizer
For severe bronchospasm give nebulizer continuously |
| Prepare for ET intubation |
If the child has hypotension:
- Put the child in supine position
- Give small boluses of epinephrine or infusion titrated amount
- Give isotonic crystalloid
|
| Give methylprednisolone or corticosteroids and diphenhydramine |
| Lower Airway Obstruction |
| Anatomy |
Obstruction in lower trachea, bronchi or bronchioles
|
| Causes |
|
| Signs and Symptoms |
- Tachypnea
- Cough
- Wheezing
- Increased expiratory effort with longer expiratory phase
- Increased respiratory effort
|
| Management |
Management of all lower airway obstruction includes:
- Slow rate with bag-mask ventilation
|
Specific causes of lower airway obstruction include asthma and bronchiolitis.
Bronchiolitis
Bronchiolitis is inflammation of the bronchioles with coughing, shortness of breath and wheezing. Management of bronchiolitis includes the following:
- Nasal or oral suctioning
- Ancillary testing – chest x-ray, arterial blood gas analysis and viral studies
Asthma
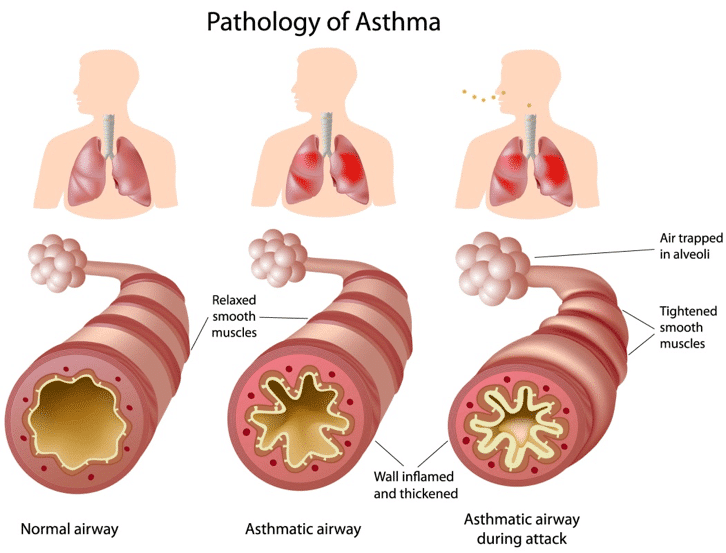
Asthma is a chronic inflammatory disease of the airway with symptoms of coughing, shortness of breath, wheezing and tightness of the chest. The following table illustrates the management of asthma.

| Lung Tissue Disease |
| Anatomy |
Clinical conditions with the lungs |
| Causes |
- Pneumonia
- Pulmonary edema
- ARDS
- Trauma
- Allergic reaction
- Toxins
- Vasculitis
|
| Signs and Symptoms |
- Tachypnea
- Tachycardia
- Crackles
- Increased respiratory effort
- Grunting
- Hypoxemia
- Decreased breath sounds
|
| Management |
Management of all tissue lung disease includes:
- Use positive expiratory pressure for hypoxemia
- Administer humidified high-flow nasal cannula
- Monitor tissue perfusion and cardiac output
|
Specific causes of lung tissue disease include pneumonia, chemical pneumonitis, aspiration pneumonitis, cardiogenic pulmonary edema and noncardiogenic pulmonary edema (ARDS).
Pneumonia
Pneumonia is inflammation of the alveoli of the lungs due to infection by bacteria, viruses, fungi and parasites. Pneumonia presents with fever, chest pain, cough, difficulty in breathing. The management of pneumonia includes:
- Antimicrobial therapy
- Albuterol by MDI or nebulizer
- Use CPAP or BiPAP
- Normalize temperature by treating fever
- Conduct ancillary testing
Chemical Pneumonitis
Chemical pneumonitis is inflammation of the lungs caused by breathing in toxic substances. Toxic substances include dust, fumes, irritant gases, hydrocarbons. Management of chemical pneumonitis is done by:
- Use of CPAP or BiPAP
- Give nebulized bronchodilator
- Consultation of a severity center
Aspiration Pneumonitis
Aspiration pneumonitis is inflammation of the lungs caused by content of the stomach such as stomach acid and enzymes. For treatment of aspiration pneumonitis consider the following options:
- Use of CPAP or BiPAP
- Administer antibiotics for fever and infiltrates
Cardiogenic Pulmonary Edema
Cardiogenic pulmonary edema occurs when there is an accumulation of fluid in the lung interstituim and alveoli because of elevated pulmonary capillary pressure. Most common cause of cardiogenic pulmonary edema is congestive heart failure and acute myocardial dysfunction. Management of cardiogenic pulmonary edema includes:
- Ventilatory support
- Medical therapy by reducing left atrial pressure, left ventricular afterload and give inotropic or inodilator therapy
- Decrease temperature and breathing by reducing metabolic demand
Noncardiogenic Pulmonary Edema (ARDS)
Acute respiratory distress syndrome is inflammation of the lung parenchyma causing difficulty in breathing, hypoxemia and multiple organ failure. ARDS as defined by the American Heart Association is, acute onset, PaO2/FiO2 <300, bilateral infiltrates on chest x-ray, and no evidence for a cardiogenic cause of pulmonary edema. Management of ARDS includes:
- Monitor the patient’s pulse oximetry, end tidal CO2, cardiac markers
- Get labs like ABG, venous blood gas and CBC
- Give continuous ventilation
| Disordered Control of Breathing |
| Anatomy |
Problems associated with the respiratory system |
| Causes |
- Seizures
- CNS infections
- Head injury
- Brain tumor
- Hydrocephalus
- Neuromascular disease
|
| Signs and Symptoms |
- Irregular respiratory rate
- Variable respiratory effort
- Shallow breathing – causes hypoxemia and hypercarbia
- Central apnea
|
| Management |
Management of disordered control of breathing includes:
- Conduct the ABC assessment
|
Specific causes of disordered control of breathing include increased intracranial pressure (ICP), poisoning or drug overdose, and neuromuscular diseases.
Increased Intracranial Pressure
Increased intracranial pressure can be caused by:
- Meningitis
- Encephalitis
- Intracranial abscess
- Subarachnoid hemorrhage
- Subdural or epidural hematoma
- Traumatic brain injury
- Hydrocephalus
- Central nervous system tumor
Proper management of respiratory distress or failure due to increased ICP includes:
- Jaw thrust maneuver
- Open airway
- Give 20 mL/kg IV isotonic crystalloid
- Give hypertonic saline, osmotic agent
- Avoid hypothermia and hypotension
- Treat agitation
Poisoning and Drug Overdose
Poisoning and drug overdose is one of the most common and frequent causes of respiratory distress in infants and children. The following actions must be taken to treat this type of respiratory distress.
- Contact the poison control center
- Administer the antidote to the poison
- Suction airway if patient vomits
- Conduct the ancillary test
Neuromuscular Disease
Neuromuscular disease is broad term that is given to various diseases that impair muscle control and causes spasticity or paralysis. Children with neuromuscular diseases which affect respiration have the following symptoms:
- Cough
- Atelectasis
- Restrictive lung disease
- Pneumonia
- Chronic respiration insufficiency
- Respiratory failure
For management of neuromuscular disease in children complete the ABC assessment, which includes supporting the airway, breathing and circulation.



